

Complex Head & Neck Skin Cancer
Managing these cases requires more than a single surgeon.
Why Mr Potter
158 neck dissections performed for metastatic skin cancer
144 skull base cases performed
0% nerve injury across neck dissections
0% stroke
0% mortality (30-day and 3-month)
0% PE/DVT
0% chyle leak
0.6% haematoma rate (1/158)
0% free flap loss in skull base reconstruction
Average hospital stay: 8 days (neck dissection); 10 days (skull base)
PHIN patient satisfaction score: 99%
PHIN is an independent government audit of consultant patient outcomes, randomly sampling post-operative patients. A 99% satisfaction score places Mr Potter among the highest-rated plastic surgeons in the country.
Our Technique
Neck Dissection & Parotidectomy
Minimising deformity — Mr Potter's technique
Skull Base Surgery
Multidisciplinary Review
All complex head and neck skin cancer cases are discussed at a Skin Cancer MDT, a Head and Neck MDT, and where appropriate a Skull Base MDT. Patients have the opportunity to discuss all available treatment options — surgery, radiotherapy, chemotherapy, and combinations — with all relevant specialities before any decision is made.
Facial Nerve Involvement & Reanimation
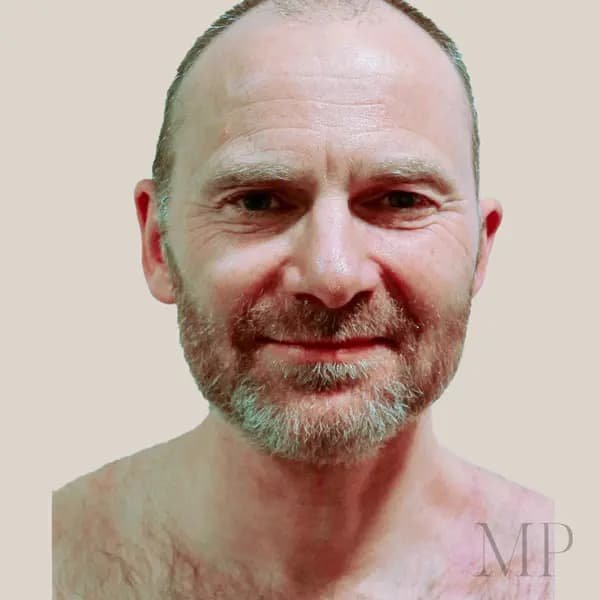
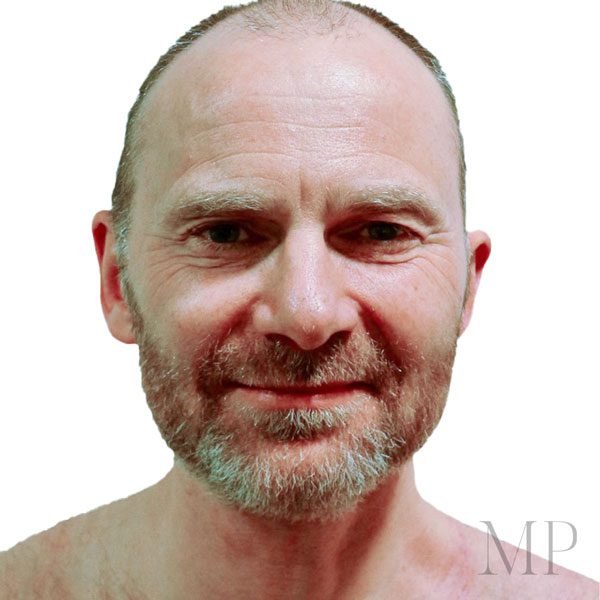
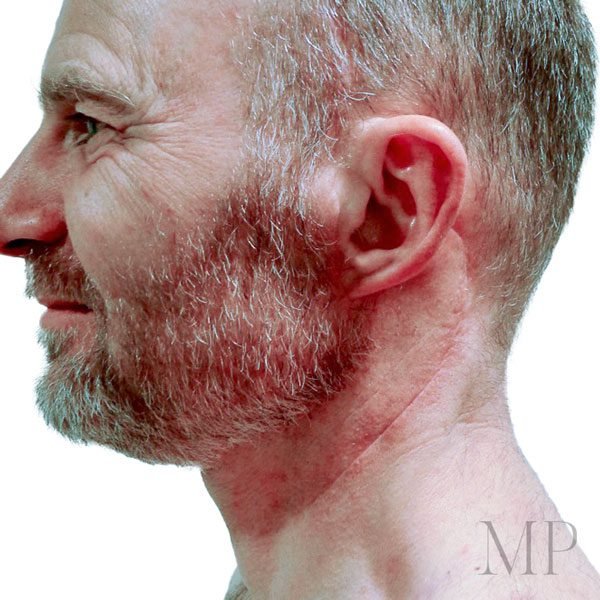
Patient Imagery


What Patients Say
Forgive the bullet points but they help to make my views clear:
- Technically brilliant – I had 2 successful cancer operations, one significant, but was left with minimal scarring and and physical changes and am cancer free at this time.
- Bedside manner – brilliant. Caring, clearly explains things, never in a rush, I felt like the most important thing on Matt’s mind when we were together and he was prompt to respond to queries when I was not.
- Mental well-being – Matt was careful to ensure that this part of my cancer and surgery recovery was not overlooked and his referral to a phsyco-therapist was important.
- Lissie Mead PA – also brilliant at her job.
- Future – I will be under Matt’s care for at least another 5 years and feel safe and happy to be so.
Thank you Matt and team.
Frequently Asked Questions
When does skin cancer require neck dissection?
When skin cancer of the head and neck spreads to the regional lymph nodes — which lie within the parotid gland and the neck — those nodes need to be surgically removed. This prevents further spread and reduces the risk of recurrence in the neck.
What is Frey's Syndrome and how does Mr Potter address it?
Frey’s Syndrome is a condition where the skin sweats noticeably when eating or feeling hungry — a common side effect of standard parotidectomy. Mr Potter uses a tissue flap to fill the operative defect at the time of surgery, specifically to minimise this and reduce the cosmetic hollow that standard procedures leave behind.
What happens when skin cancer invades the skull?
When skin cancer invades the skull or skull base, the involved bone is excised and reconstructed using a custom cranial implant or titanium. The overlying skin defect is reconstructed using local tissue or, for larger defects, a muscle transplant from elsewhere in the body. These cases are managed by Mr Potter working alongside ENT and neurosurgical colleagues.
Can facial palsy be reversed after facial nerve sacrifice?
In many cases, yes. Mr Potter performs dynamic facial reanimation using a free flap technique — transplanting tissue and rewiring the facial nerve so that the affected side learns to smile. His series records 100% return of facial movement at six months, across all ages including patients in their 80s.
Will my case be reviewed by a specialist team?
Yes. All complex head and neck skin cancer cases are discussed at a Skin Cancer MDT, a Head and Neck MDT, and where appropriate a Skull Base MDT. All available treatment options are considered before a plan is agreed.
Where does Mr Potter perform head and neck skin cancer surgery?
Complex head and neck cases are performed at specialist hospital facilities alongside ENT, neurosurgical and skull base colleagues. Mr Potter will advise on the relevant location during consultation.
Book a Consultation
Contact us if you have any health concerns or are looking to get a consultation. You can contact Matthew Potter by using the form below or contact him through one of the available telephone numbers or email addresses listed on this page.
Private Secretary & All Correspondence
T. 07917 965717
Swindon - Ridgeway Hospital
T. 01793 814848
Cheltenham - ProDerm, Festival House
T. 0800 0489230
Oxfordshire - Stratum Clinic,
Wootton Business Park
T. 01865 320790
Wiltshire - Interface Business Park, Royal Wootton Bassett
T: 0808 2803560
Oxford - The Manor Hospital
T. 01865 307777
Contact Lissie on 07917 965717 or use the form below.